



Chapter 5
What we found: Heredity
What you’ll learn in this chapter
In this chapter, we’ll cover:
- How heredity works;
- Some factors that make people diverse, such as biological sex, gender identity, and genetic ancestry / ethnicity; and
- Why our history matters, and why we have to consider ancestry when understanding and interpreting genetic data.
As you read this chapter, remember our usual caution:
As with most preferences, health risks, and genetic traits, there are many complex, interrelated factors.
There is almost never one single gene that inevitably leads to a given result.
Any genetic data we share are simply clues for further exploration.
It all begins with sex.
Humans reproduce sexually, which means one cell’s genetic information has to hook up with another cell’s genetic information to make a new human.
In this process, genetic traits are passed on from parents to child. You might inherit your father’s nose, or your mother’s curly hair.
But this doesn’t mean we are exact clones of our parents. Gametes (the chromosome-containing cells we get from our mom, an egg/ovum and dad, a sperm) combine in ways that we can’t completely predict.
Gametes are haploid, which means they each have only one copy of the 23 chromosomes that make up the human genome. (The word “haploid” comes to us from the ancient Greek haploos, or “single, simple, once”.)
When the haploid egg and sperm cells unite, they eventually create a person with diploid cells — twice the amount, or 46 chromosomes. (The prefix “di” refers to two.) So, aside from our own sperm or egg cells, the rest of the cells in our bodies have 46 chromosomes.
How does heredity work?
Heredity is complex. Given all the DNA in our genetic code, and given that we get stuff from mom and dad, there are almost infinite possible combinations of traits.
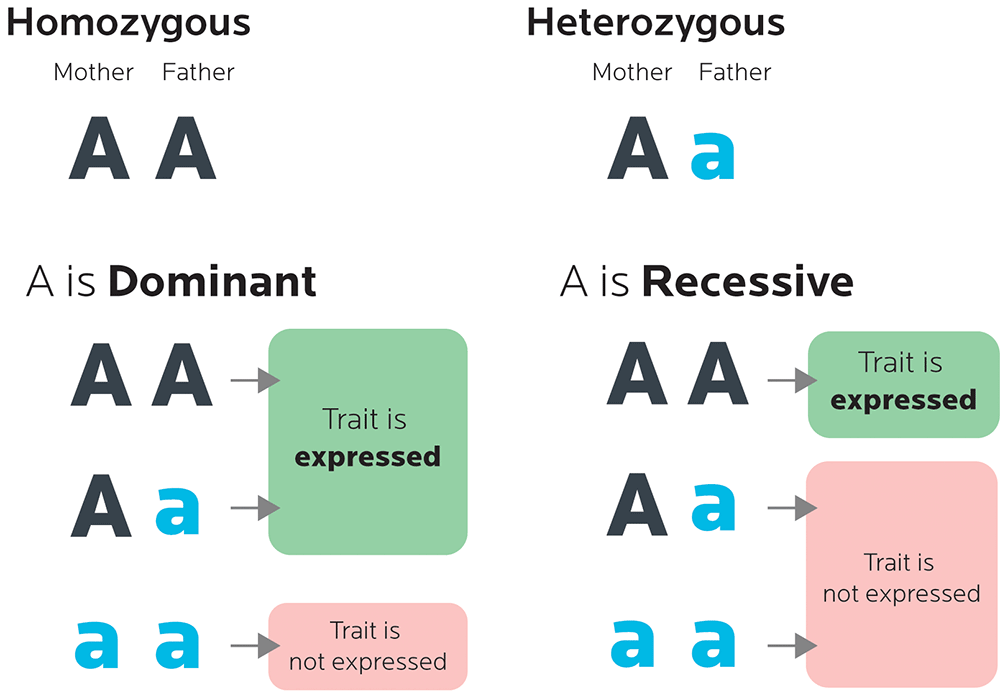
Some traits are dominant, meaning they are more likely to be expressed. Some traits are recessive, meaning that they are less likely to be expressed. We might need to inherit two copies of a recessive gene in order to express it, whereas we might need only need one copy of a dominant gene.
- If we have two copies of a particular gene type, that’s called homozygous.
- If we have one copy of one type, and a different copy of another type, that’s called heterozygous.
Interestingly, many traits that are supposedly one-gene, or monogenic, traits (like eye color or the curvature of your thumb) are not. Instead, they are polygenic, controlled by multiple genes.
In our PN population sample, we included some multi-generational data: grandparents, parents and children. And since the parents surveyed had more than one child, we were also able to see how particular traits appeared in different offspring.
For example:
There is a gene that makes people more or less likely to think that fresh cilantro (aka coriander, a herb often used in Latin American and Asian cuisines) tastes yucky (which we’ll look at in Chapter 8, on food preferences).
Part of this gene can come in 3 nucleotide combinations:
- AA (adenine-adenine): More likely to dislike cilantro
- AG (adenine-guanine): So-so
- GG (guanine-guanine): Less likely to dislike cilantro
In our sample, we found different types of inheritance.
Parent-child group 1:
AG mom + AG dad = 2 GG children
Parent-child group 2:
AA dad + GG mom = AG child
Parent-child group 3:
AG dad + AG mom = 2 AG kids
And, as you’ll see in Chapter 8, just knowing a person’s genetic makeup (i.e., their genotype) doesn’t necessarily tell us what traits they express (i.e., their phenotype). As it turns out, the “cilantro-hatin’ gene” didn’t predict which of our PN sample actually hated cilantro.
What this means for you
- Genetic testing can tell you about what traits you may have inherited.
- However, you may not necessarily express those traits.
Biological sex is complex.
Ova have only an X chromosome, while sperm can have either an X or a Y. Most of the time, males have an XY chromosome combination, while females have an XX combination.
This combination of chromosomes is what gives us our biological sex — our collection of physiological characteristics that we might call “male” or “female”.
Biology is rarely so completely neat and tidy, though. Sexual dimorphism (i.e. being able to divide a species into two sexes by their physiological characteristics) does not mean that male and female bodies are “opposites”. Rather, it’s a bit more like biological sex is on a continuum. It’s quite possible, though less common, to have other combinations of chromosomes.
For example:
- A body can have XY (i.e. biologically male) chromosomes, but for other genetic reasons (such as variations on other related genes), develop a female body. Testes don’t descend while XY fetuses are in the womb, so when they are born, they might look like any other baby girl. Often this has to do with insensitivity to the masculinizing hormones, known as androgens. Many XY women do not discover they are unusual until they hit puberty and don’t menstruate.
- Similarly, a body can have XX (i.e. biologically female) chromosomes but look male during development. Typically this happens when haploid chromosomes are created, and a Y-chromosome SRY gene (which contributes to masculinized development) sneaks in from dad and ends up on another chromosome.
- Many bodies can also inherit additional chromosome copies, such as XXY, XXX, XYY, and so on.
In general, these types of phenomena, where bodies are chromosomally or developmentally sexually ambiguous (or both), are often known as intersex. It’s estimated that about 1 in 1,500-2,000 people are intersex in some way.
All you need to remember is:
Biology is complicated.
As is identity. We’ll look at ethnicity in a moment, but first, a quick detour.
Is transsexualism genetic?
One of our co-authors, Alaina, has an interesting feature: She’s transsexual. (We also had one more trans woman in our genetic sample.)
Nobody knows exactly how common it is to have some type of “mismatch” between one’s biological sex configuration (i.e., chromosomes and other physiological characteristics), and one’s gender identity (i.e., one’s sense of self as having a particular gender, or not).
But both gender variation and intersex are common enough that we now ask about it on our PN Coaching client intake form:
Which sex/gender do you most identify with:
-
- Man
- Woman
- Other
If other, please specify: _______________
Biological sexual characteristics (such as hormones) can affect people’s metabolism, nutrition, and response to exercise. Gender identity affects who they are in the world. We consider these important things to know about our clients, so that we can take the best possible care of them.
Given the ways that chromosomal inheritance can work, intersex is a fairly clear-cut phenomenon. It’s simply a normal (though relatively infrequent) variation of sexual development with a clear mechanism of action.
But what about gender identity? In other words, who we feel we are, at a deep level? Could genetics play a role here too? Possibly.
For instance, some evidence suggests that genes involved in the production and function of sex hormones may be important, such as:
- androgen receptor genes (AR or NR3C4);
- estrogen receptor β genes (ESR2 or NR3A2); and
- aromatase (CYP19) genes (genes involved in aromatization, or conversion of sex hormones, such as from testosterone to estrogen).
Two studies, for example, found that female-to-male transsexuals were more likely to have variations in the CYP17 gene (which encodes 17α-hydroxylase, an enzyme involved in conversion of sex hormones.) Other research found no such association.
Another study, yet to be reproduced, looked at the gene (AR, or NR3C4) that codes for the human androgen receptor.
Androgens are a group of sex steroid hormones that are considered to be biologically “masculinizing” hormones, though they appear in all human bodies to some degree. Testosterone is the best-known example, but there are others, such as dihydrotestosterone (DHT) and androstenedione.
Androgens and other hormones bind to receptors on cells to do their job. This means that if receptors vary genetically (for instance, if they are shaped differently, or more or less active), this can affect hormonal function.
The AR gene has several variants where a stretch of 3-nucleotide codons with the makeup of cytosine + adenine + guanine (giving it the acronym CAG) is repeated different numbers of times. This is known as a variable number tandem repeat (or VNTR).
For example, you might see this on some people’s AR gene:

You might see this on other people’s AR gene:

The study looked at how often each variant, or allele, appeared in a study population of both transsexual women (male-to-female) and non-transsexual men, and found that there might be a link between certain alleles of AR and being transsexual. Male-to-female transsexuals were more likely to have a particular number of tandem repeats in the AR gene.
As it turns out, Alaina does, indeed, have this variation. (We didn’t test the other woman’s full genome, so we don’t know if she does.)
What this means for you
- A possible genetic correlation with gender identity is interesting in its own right, and perhaps validating for many trans people. If these kinds of results could be replicated and more solidly established scientifically, it might help demonstrate (at least, for some people) that their deeply felt sense of being a particular gender has at least some biological roots.
- More broadly speaking, variations in genes and structures that affect sex hormones might also:
- offer possible drug therapies. For instance, changing the function of an androgen receptor could also offer treatment for prostate cancer.
- affect body composition. For instance, men who more easily convert (aromatize) testosterone to estrogen may have trouble losing body fat.
- affect athletic performance and, potentially, drug test results. For instance, women with naturally higher-than-average androgen levels may build muscle more easily. In extreme cases, elevated androgen levels in some women who are intersex (such as the famous cases of female sprinters Caster Semenya and Dutee Chand) may cause them to fail drug tests. We’ll look more at other genes that may affect exercise, muscular performance, and body composition later in the book.
- Though you can do a chromosome test to determine biological sex, most commercial genetic tests do not (yet) test for variants related to gender identity. Our data came from a full-genome sequence.
- Nor, by the way, can you currently test for sexual orientation. 23andMe also looked for variants that might be related to sexual orientation — in other words, whom we prefer as sex partners. Using a survey of nearly 24,000 people, they eventually concluded that there were no clear links between any SNPs and sexual orientation. Genetic data in this area, while intriguing, are still inconclusive and don’t yet represent the full range of human behavior.
Our history is complex.
Along with our physiological sex, part of what makes “us” us in biological terms is our ancestry, ethnicity, and heritage.
Where do you come from? Where are your roots? Who were your ancestors?
Of course, the first answer is that all of us descend from a relatively small population of hominins (or early humans) who began their journey in Africa.
Once they could stand upright, those adventurous, ancestral primates started walking. And walking. And walking. Eventually they spread around the globe, mutating and evolving and turning into a vast rainbow of humanity.
And now those curious little walking primates are us.
The second answer explains more recent history: Where have your ancestors been for the last several thousand years? Where have they traveled? Who did they meet, and marry, and trade with? (Did someone else trade them?)
How might someone recognize you (or not?) as being “from somewhere”, perhaps a particular place on Earth, or a particular group of people? What traits do you have that might be a dead giveaway… or a mystery?
Almost all of us writing this book, and from the PN team who consented to let us use their data, are from European backgrounds.
For instance:
- John’s family is originally from Italy.
- Helen’s family is originally from Greece.
- Alaina’s ancestors are originally from England, Ireland, Scotland, and Germany. Most of her family came to the United States between 1635 and 1650. Her Scottish ancestors landed in 1879.
- Krista’s family is a mix: part Northern European; part Eastern European; and part Southern European (particularly the Balkan region).
The one exception:
- Our PN team member Tim’s ancestry is about half European and half South Asian, with a bit of Sub-Saharan African (mostly West African) thrown in.
Our history can tell us about ourselves.
When clients start our PN Coaching program, we ask them about their ethnicity. People can tick as many boxes as they like.
Here’s the list we use:
-
- White/European
- Black/African American
- Hispanic
- East Asian
- South Asian
- Pacific Islander
- Arabic/Middle Eastern
- North American Aboriginal/First Nations/Native American/Inuit
- Aboriginal Australian
- Other (please specify)
Many clients wonder:
Why do we ask about this?
The simple answer is that aside from social and cultural traditions, our ancestry and ethnic origin are really just a way of saying “genetically-related groups”. Genetically-related groups tend to inherit particular traits.
The traits we inherit may in turn affect things such as:
- our food choices;
- our response to diet and exercise;
- our food intolerances and sensitivities; and
- our health risks or advantages.
But in reality, there is no simple answer.
- Heredity is complex. (After all, you get stuff from mom, and stuff from dad, and these days you might get stuff from a third person because why the heck not!? Science! See below for more.)
- Ancestry is complex.
- Ethnicity is complex.
- How all of these affect your nutrition, exercise, and health is complex. (Remember, other biological, social, and environmental factors are still in the mix too.)
And that’s what we’ll look at in this chapter.
How can a child have 3 parents?
The “3-parent” artificial reproduction technique was first done successfully in 2016, and is used to lower the risk of genetic diseases in mitochondrial DNA if there is a known concern.
There are a few ways to do this.
One method, known as pronuclear transfer, uses two fertilized eggs, both fertilized with the father’s sperm: one egg from the mother, and one egg from a donor.
Once eggs are fertilized, but before they start dividing, their nuclei are removed. The nucleus from the donor’s fertilized egg is replaced with the nucleus from the mother’s egg.
A second method, known as spindle nuclear transfer, is similar, but the swap occurs before fertilization.
In this case, doctors purposely created and used a male embryo, so that the resulting child wouldn’t pass on any inherited mitochondrial DNA. (Thus, the genetic disorder would end.)
We’ll read more about mitochondrial DNA later in this chapter.
Genetic data tell us there is no such thing as “race”.
At least, not in the way most people think about it, which is a few very simple categories. Instead, genetically speaking, there are only ethnic subgroups or common groups of genetic variations that can be loosely distinguished.
History tells us that humans have always been nomadic people. We’re social — we like to meet ‘n’ greet (even if sometimes that “greet” is with a whackin’ club to drive off the other tribe).
We humans like to travel and trade. Some folks wandered up and out of Africa. Some folks wandered all the way across Alaska to South America. Some of us even got gutsy enough to take a raft across the ocean, resulting in relatively historically isolated and genetically distinct populations such as indigenous Aboriginals in Australia, Torres Strait Islanders, Maori, and Indonesians.
Once we figured out walking, riding, and sailing, we got busy swapping and selling stuff like spices and silks and — appallingly, shamefully, and horribly — sometimes, other humans too. (There is evidence that enslavement, sale, and other forced migrations of humans happened all over the world, and goes back at least to around 3,000 BC. Tim’s great-grandparents were brought to Trinidad as part of human trafficking routes from India and Africa.)
This means that unless you and your ancestors have lived for tens of thousands of years undisturbed in some pocket of the Amazon, an isolated mountain pass, or a desert island that has yet to be turned into an all-inclusive resort, you’ve probably got a buffet of mixed-up human DNA inside you.
For instance:
- Although John’s DNA is about 97% Southern European, he’s got about 3% from North Africa, reflecting patterns of migration and the influence of Arabic trading with the Mediterranean. He’s also got maternal and paternal lineage of a type most common in the Middle East.
- Krista has a smidge of East Asian, possibly from the dominant Mongol Empire that swept through the Asian and eastern European continent in the 13th and 14th centuries. In fact, genetic testing estimates that 1 in 200 men in the world carries this lineage.
- Tim’s DNA is about 1/4 Ashkenazi Jewish, a population of European Jews who tend to be closely related as a relatively historically insulated community. Even more interesting: Tim’s mother (of European descent) hadn’t known.
We are all connected. We are family.
Europeans, East Asians, and Neanderthals
Evolution is rarely nice and tidy. There are lots of branches, dead ends, and false starts.
Genetic data can tell us about our complex journey to modern humanity, as well as about our closest relatives both living and extinct.
Though we might imagine we evolved in a clear, straight line from primate to Homo sapiens (i.e., you), it didn’t actually happen that way. In fact, we co-habited with many types of hominins as recently as 100,000 years ago. Our ancestors (like the ancestors of most other species) branched into many now-extinct subspecies, such as Homo naledi and Homo florensis (aka “the hobbit”).
Though Neanderthals are a distinct evolutionary branch of the human family, and disappeared around 40,000 years ago, they got in a few good romantic moments with our Homo sapiens ancestors before they disappeared.
This means that many people of European ancestry carry at least a little bit of Neanderthal DNA — between 1-3% of their total. However, one study on a sample from a modern human who lived in what is now Romania between 37,000 and 42,000 years ago contained about 6-9% percent Neanderthal genetic material, more than any other modern human genome that has yet been sequenced.
This isn’t the whole story, though. Research also suggests that the ancestors of present-day East Asians split from Europeans, then interacted later with Neanderthals.
In other words, it wasn’t a simple process of a single meeting — there were many complex patterns of genetic mixing with different populations over the course of early human history.
Krista scores 96th percentile for this genetic material; John 67th; and Alaina 38th. If you’ve got European or East Asian ancestry, you likely have at least a little Neanderthal in you.
Ethnic variation within a region
The 1992 film White Men Can’t Jump, starring Woody Harrelson and Wesley Snipes, played on the idea that white athletes would be lousy basketball players. Indeed, “black” and “white” are easy, simple categories, often used to divide and explain the world, whether in terms of ethnicity, ability, perspective, or other physical and cultural differences.
In reality, these terms are not at all simple.
They’re complex, laden with historical baggage, and change in subtle but important meanings from place to place (for instance, “Black” historically meant somewhat different groups of people in North America, South Africa, or the UK). And they don’t tell us much about many important features of people.
For now, let’s set aside social and political issues of ethnicity, and look at the physiology.
On one hand, we are all human.
We are more alike than we are different.
And we are more alike than other species — for instance, there is more genetic variation among fruit flies than among humans.
On the other hand, many distinct traits or genetic variations can be reproduced within populations.
This is especially true if those populations have traditionally tended not to travel much, or marry “outsiders”.
We can safely expect, for instance, that an Indigenous person from Australia — whose ancestors arrived on the island about 50,000 years ago — will likely be measurably different than an Indigenous person from an isolated mountain village in Chile — whose ancestors may have crossed the now-vanished Siberian land bridge across the Bering Strait (between Russia and Alaska) approximately 30,000 years ago.
Some traits (such as facial features or body shape) may be easy to see. Others, such as immune system variations, may not be.
On the other other hand, some regions have significant genetic variation and ethnic subgroups.
Somewhere around 1.5 to 2 million years ago, a group of early hominins from Africa walked north and gave rise to most of modern humans. But other hominins, of course, stayed.
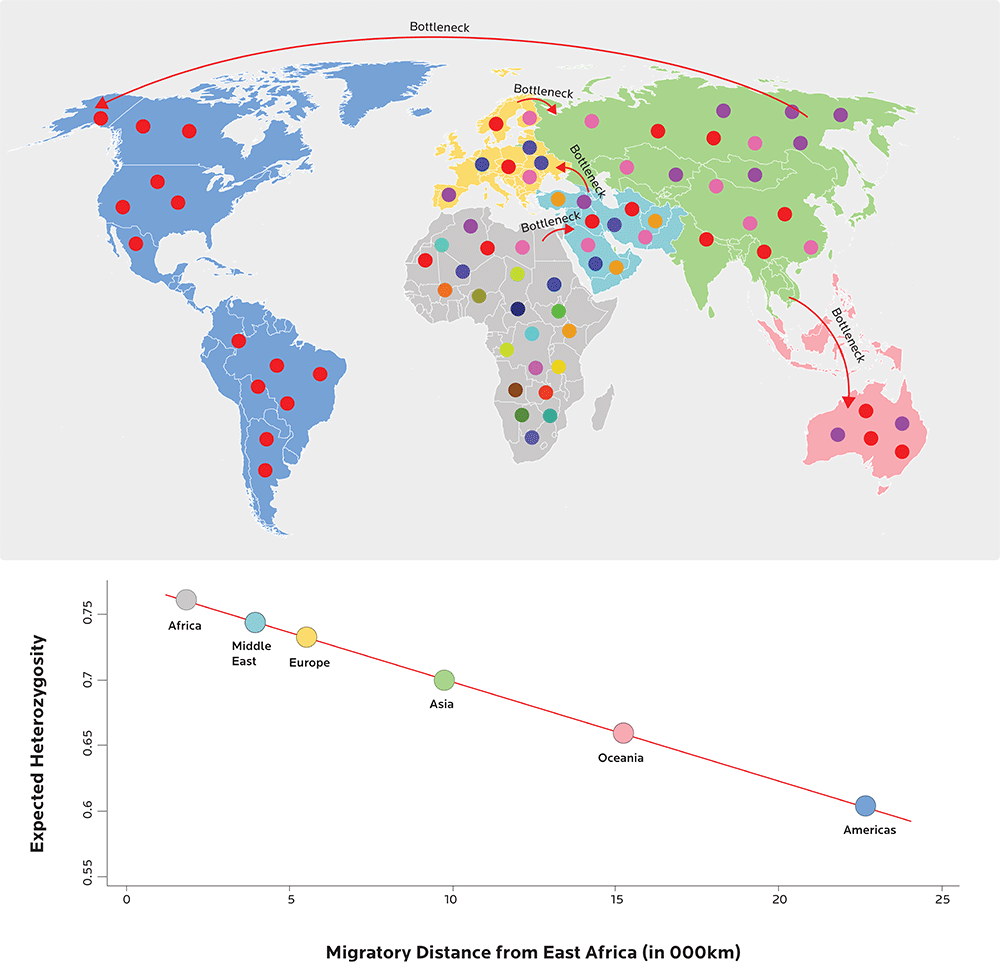
Thanks to this ancient lineage, the massive continent of Africa is one of the most genetically diverse regions in the world.
For instance, one study found that the average nucleotide diversity was twice as high among Africans as among Europeans and Asians. North Africans are genetically distinct from sub-Saharan Africans, since the Sahara Desert would have been a barrier that few crossed before modern means of transport. The further from East Africa early human populations traveled, the less genetically variable they tended to become.
However, areas with lots of trade (such as the Mediterranean or the Malaysian peninsula) were perfect environments for population and genetic material exchange. Not surprisingly, there is more genetic diversity in southern than in northern Europe, which is further away from the busy shipping routes between the Middle East, Asia and Africa.
Yet even some small regions such as northern Europe have at least a bit of diversity — evidence suggests that multiple waves of early humans ebbed and flowed into the northern regions of Europe as Ice Ages came and went. And Melanesia (the area northeast of Australia that contains Papua New Guinea, Fiji and other small Pacific islands) has significant genetic diversity.
So being “white”, “European”, “black”, “African”, or any other ethnic category, is not a simple thing at all.
We’ll see this when we look more closely at specific responses to nutrition and exercise in the upcoming chapters.
What this means for you
- By virtue of being human, you contain complexity. Genetics is not simplistic, nor are physiological categories like “sex” or “ethnicity”.
- Genetic testing can tell you about your history, which may be more diverse than you anticipated. After all, your ancestors had lots of time to mix things up.
- You’re not “destined” to be anything in particular just because of biological sex or genetic ancestry. Genetics can only tell us about probabilities and relative frequency of particular instructions for making proteins.
How can you trace your lineage?
The words “haplotype” and “haplogroup” come to us from the same ancient Greek root as “haploid”.
We can think of haplotypes as something like a cluster or constellation of genes (in other words, a small chunk of genetic material) inherited together from a single parent, and a haplogroup as a group of closely linked haplotypes that tend to be inherited together.
Generally, haplogroups can be traced back to a single line of descent from a common ancestor.
Mom’s lineage: Mitochondrial DNA
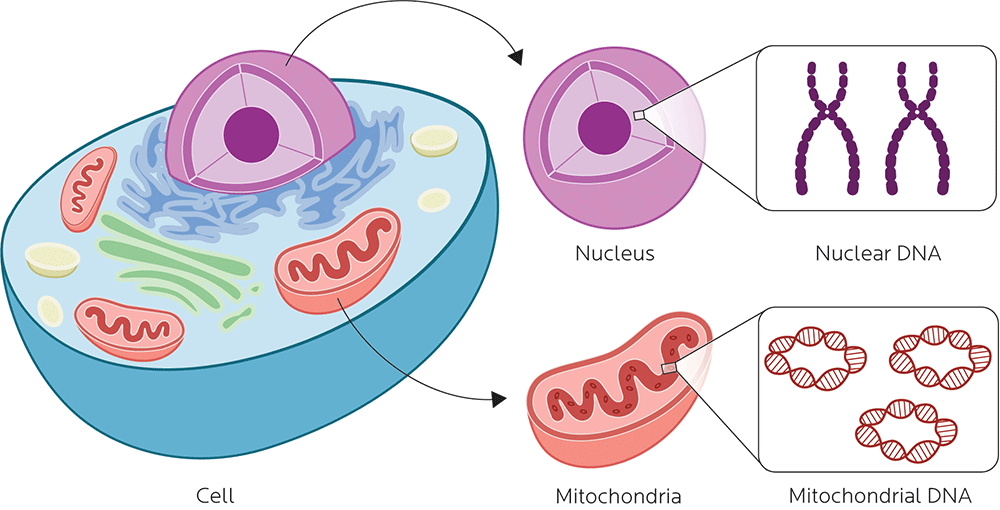
Mitochondria are organelles (cell components) that convert energy from food into a usable form (in humans, that’s adenosine triphosphate, or ATP).
Mitochondria have their own DNA (aka mtDNA) that is distinct and independent from the 46-chromosome DNA of a cell’s nucleus. There isn’t a lot in there — only 16,569 base pairs of mitochondrial DNA that code for only 37 genes — but this relatively small snippet of DNA can tell us a lot about ourselves.
Many people have wondered why we have mtDNA, and why the mitochondrial chromosome is circular, like a bacterial chromosome.
MtDNA does seem to be related to certain species of modern bacteria. Many of the former-bacteria’s genes encode for the stuff specifically related to the function of the mitochondria. Some even seem to have been transferred to the host organism’s genome.
Mitochondria were likely originally bacteria that invaded the ancestor(s) of eukaryotic cells (i.e., cells with a nucleus and organelles) and developed a symbiotic relationship. The resulting friendship was a common ancestor for an entire domain of life: the taxon Eukarya, which includes plants, animals, fungi, algae, and many single-celled organisms, such as amoebas.
In humans, while sperm cells have mitochondria, they seem to get destroyed by the egg after it is fertilized. We usually inherit mitochondrial DNA only from our mothers, not our fathers.
So by categorizing mtDNA and looking at where it’s spread in the world, we can retrace the footsteps of our female ancestors.
Fun factoid!
Mitochondrial DNA inheritance is rare but does happen in some species, such as bivalve molluscs. And, to date, it has been discovered in a human male.
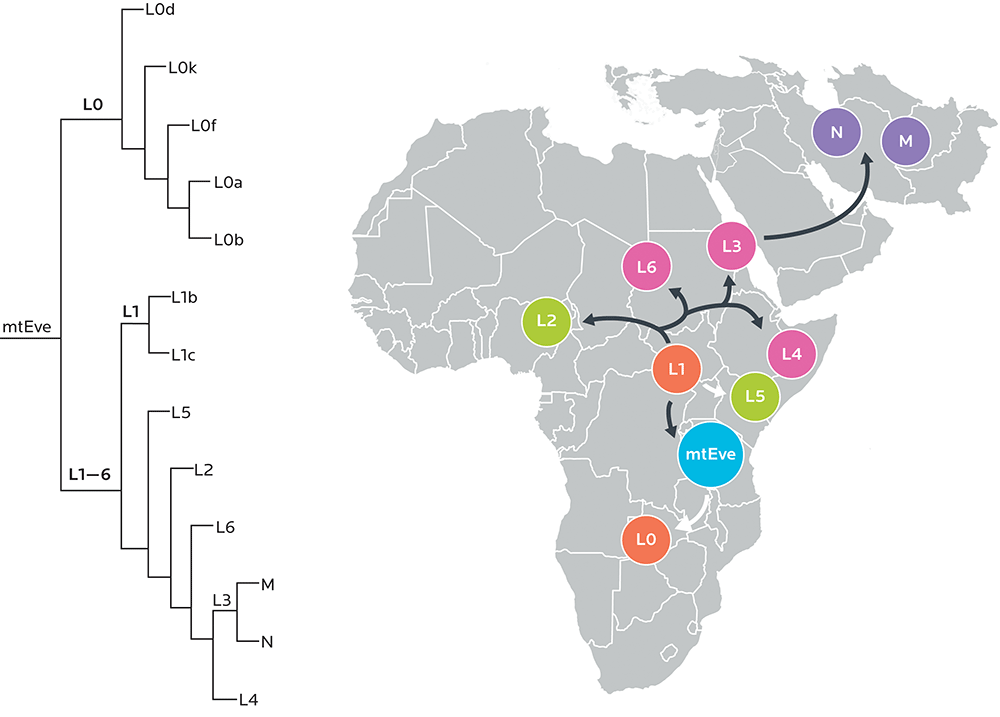
These clusters of mtDNA — which generally share a single mutation that happened to a particular ancestor at a particular place and time — are known as maternal haplogroups.
We can trace our maternal ancestry back to a woman known as “mitochondrial Eve”, a woman who lived around 190,000 years ago in East Africa. (Tanzania has both high genetic diversity and ancient mtDNA haplogroups, many of which are either uncommon or not found in other parts of Africa.)
Mitochondrial Eve gave rise to the L haplogroups, which formed the basis for all others, and which eventually branched into other haplogroups spread all over the world. Later, nomadic humans returned to Africa, bringing fresh haplogroups (such as H, U6, X1 and potentially M1) back to the homeland.
Dad’s lineage: The Y chromosome
Of course, you’re wondering what great-great-great-grandpappy was up to.
Paternal haplogroups are families of Y chromosomes that, like maternal haplotypes, can be traced back to one mutation that happened at a particular place and time, and, likewise, help us see the pathways our male ancestors took.
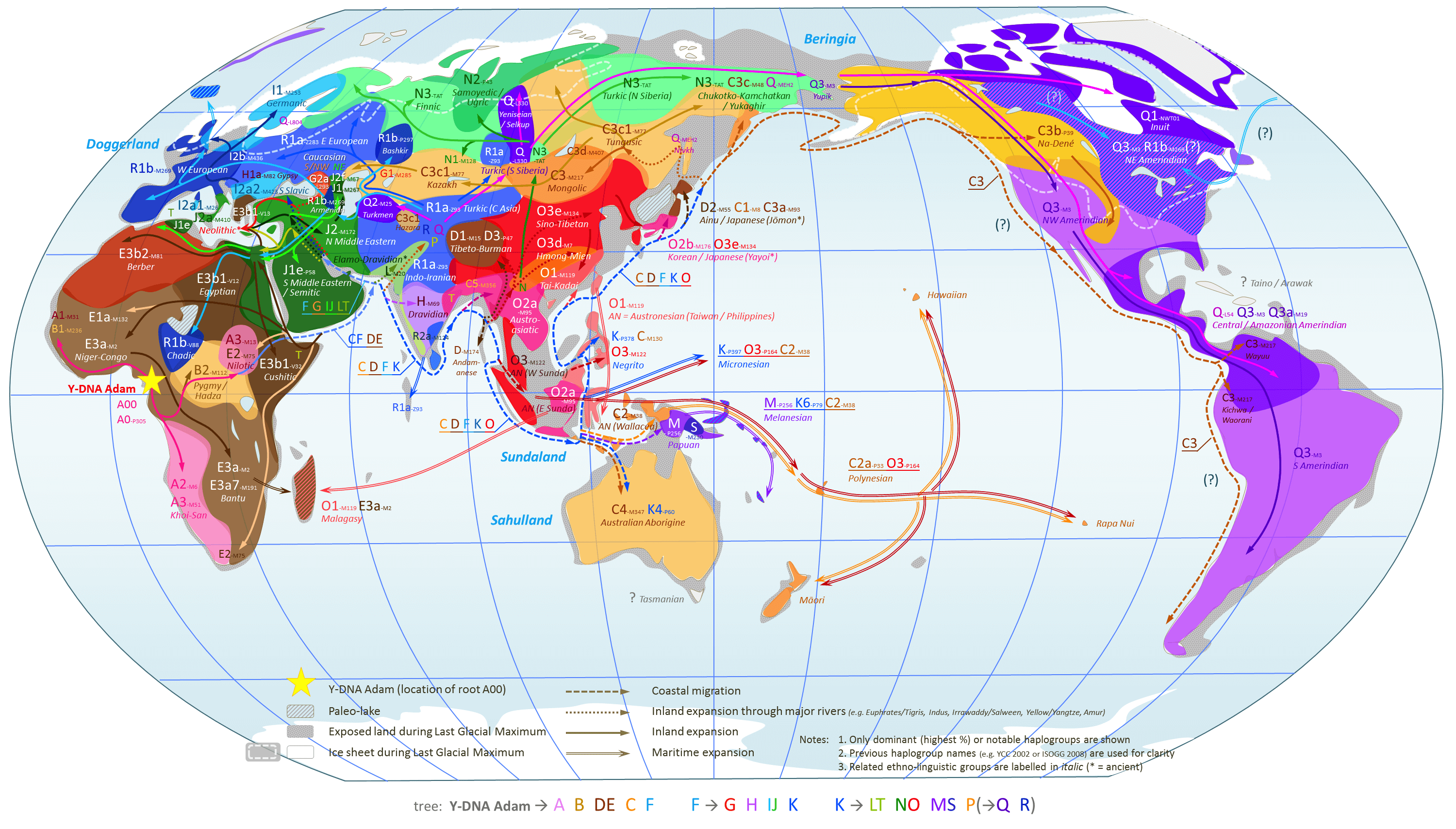
Image credit: Chakazul. World Map of Y-Chromosome Haplogroups – Dominant Haplogroups in Pre-Colonial Populations with Possible Migrations Routes. Available via Wikimedia Commons.
However, we’ll only see paternal haplotypes in folks with a Y chromosome (i.e., most males).
The Y chromosome is the shortest chromosome.
Though it has few genes — including the crucial SRY gene (aka testis-determining factor or TDF) — these genes are important. They code for things that masculinize bodies, such as developing testicles and producing sperm. The Y chromosome also carries many duplications and noncoding genes or transcripts.
Male infertility is a complex phenomenon (and also depends on factors such as health, medication use, nutritional status, body fat, and so forth). It can also have a strong genetic component that may include mutations to Y chromosome material.
What we found in our sample
As expected, most of our sample’s haplogroups were European. But, as we’ve seen with ancestry, things can get complicated. Maternal ancestors migrated; branches of haplogroups spontaneously emerged.
So, as with being “African”, to be “European” is not a simple thing, genetically speaking.
Here are just a few examples.
Haplotype I
For instance, Tim’s maternal ancestor haplogroup, I, was known to migrate into southwestern Asia as well as into northern Europe (some speculate that it was carried by the Vikings).
His specific haplogroup, I2, is relatively young, perhaps a few thousand years old. I2 traveled with a woman out of Iran and the Middle East through Anatolia and into Europe, where it’s now predominantly a European haplotype.
Conversely, his paternal ancestor haplogroup, H-M69, is an ancient one, around 50,000 years old, originating in South Asia.
Haplotype H
Krista’s maternal haplogroup is H, originally a Southwestern Asian group about 20-25,000 years old.
Antecedents of this group (haplogroups HV and R0) have been found throughout the Middle East and northern Africa, including in samples from ancient Mesopotamian civilizations as well as Egyptian mummies.
R0 has also been found in over half of bone remains from a large pre-Bronze Age settlement from around 4300-4000 BC, known as Trypillia, which today is in central Ukraine… more or less where Krista’s maternal grandfather was from.
John has a later version of the H group, known as H5a1, which may have emerged around 5,000 to 8,000 years ago in the western Caucasus or Near East (for example, Syria or Lebanon).
Haplotype U5a1a
Meanwhile, Alaina carries another relatively young haplogroup: U5a1a, which is between 8-16,000 years old, and commonly found in far northern Europeans, particularly Scandinavians.
Although U5 is mainly a European haplogroup, it has been found in the mitochondrial DNA of a 6th-century AD Chinese chieftain.
What this means for you
- You’ve inherited some stuff from your mother, and some stuff from your father. We can trace your mother’s ancestry through mitochondrial DNA. If you have a Y chromosome, then we can also trace your father’s ancestry.
- Genes tend to travel in groups. If you share some known traits with your populations of ethnic origin and ancestry, you’re more likely to share others. But this isn’t for sure; it’s just a probability.
- If you are male and concerned about infertility, genetic testing may be able to tell you if particular genes on the Y chromosome are involved. However, there are many other factors that go into determining fertility for both men and women (such as nutritional status, stress, etc.).
- This is pretty cool, right? Knowing our origins and our roots can give us a sense of wonder and pride about who we are, and how we got here. Many people from ethnic groups who have been socially marginalized find that learning about their ancestry and heritage gives them a stronger sense of identity and purpose. We can also link ourselves to the larger human family.
How does ancestry affect health?
Another reason that we ask our clients about their ethnicity is that many chronic health concerns and diseases, such as cardiovascular diseases, neurodegenerative diseases, or Type 2 diabetes, are not equal-opportunity employers. Instead, they seem to appear at different rates in different ethnic groups, populations, and regions.
For example:
- People of South Asian descent (i.e., originating from the Indian subcontinent) tend to have higher rates of visceral adiposity (fat around the middle) and higher rates of Type 2 diabetes.
- Indigenous people (e.g. Inuit, First Nations, Native Americans, Maya, Australian Aboriginal, etc.) from many regions have higher rates of chronic metabolic diseases, such as obesity, CVD, and Type 2 diabetes, especially when they eat modern Western diets that are heavy in processed foods.
- People of Ashkenazi Jewish descent, a particular European population that has tended to be insular and inter-marry, often carry a higher risk of recessive-linked diseases as well as genetic markers for diseases such as Crohn’s and breast cancer.
This relationship is not straightforward.
For instance, black men in the US have higher rates of cancer than other ethnic groups, but the same is not true for women. However, both black men and women in the US are more likely to die of cancer.
What does this reflect?
Sex differences? Differences by genetic ancestry? Lifestyle differences? Other factors, like access to health care and cancer screening? Socioeconomic and political factors, like being marginalized or confronting daily discrimination?
The answer is probably all of the above, and more.
Here’s just one example.
Heredity and the (failed) hypertension hypothesis
One of the more contentious topics in the field of heredity and ancestry was a hypothesis about why people of West African descent now living in North America and the Caribbean are more likely to have high blood pressure (aka hypertension).
As early as the 1960s, epidemiologists began to observe that on average, black people in North America and the Caribbean had nearly twice the level of clinically defined hypertension as many white populations of European descent living in the same areas. Yet black people from various populations in Africa (in other words, people who were relatively genetically related) did not seem to have the same high blood pressure.
Why the disparity?
And did this difference truly represent a “racial divide”?
In the late 1980s and early 1990s, some researchers proposed what came to be known as the “slavery hypothesis”. This theory suggested that Africans taken from their homeland and transported to the slave-based economies of the early Americas and the Caribbean became a genetically distinct group — those who survived a long and dangerous trip across the ocean, imprisoned in slave ships, often without adequate food or water.
The idea was that people with bodies that retained salt better might be more likely to survive dehydration, starvation, and illnesses such as diarrhea, vomiting, and fevers. Those few people who survived may then eventually have passed along those genes once they arrived at the destination.
In one sense, this is a scientifically attractive hypothesis — it seems logical, it points to a large-scale social phenomenon that may have created biological changes in a distinct population, and it may help explain underlying factors for chronic disease. A body that processes electrolytes (such as sodium) in certain ways may indeed be more predisposed to high blood pressure, which is (in part) related to the physiology of fluid and electrolyte balance.
However, the hypothesis was roundly criticized by other researchers, who pointed out things like:
- Some groups of white Europeans (such as Finns) also had higher-than-average blood pressure.
- Within Africa as a geographic region, there is tremendous genetic diversity (as we’ve seen).
- People of African descent, particularly in North America, have higher rates of other chronic diseases as well, such as cardiovascular disease or diabetes. As these diseases are polygenic — in other words, many genes contribute in complex and interacting ways — this can’t be explained by a single gene or even a small cluster of genes.
- Blood pressure is a complex physiological state that depends on many factors, of which sodium processing is only one.
- Most importantly, when researchers looked for genetic markers of hypertension in African American populations, they found none. Instead, the main factors that correlated with high blood pressure were age, body size, and birthplace.
Scientifically, this hypothesis, while convenient, is invalid. Nor is it supported by evidence.
Instead, social factors seem to account much more for high blood pressure and other chronic diseases, particularly in the United States.
These factors include:
- Residential segregation (i.e., different groups in different neighborhoods), which may expose black people to more environmental toxins.
- On average, compared to whites in the US, black people in the US have less access to quality health care, and higher levels of poverty. They may be more likely to smoke and drink, have poorer diets, and less access to fresh, healthy foods.
- Most importantly, social factors such as racism and stress are strongly linked to chronic diseases.
So, being of African descent and living in North America may indeed be linked to high blood pressure or other chronic metabolic diseases — but not necessarily for genetic reasons.
Why is this story important?
It reminds us that simplistic ideas about “race” are incorrect.
It helps us understand how ancestry, genes, and disease risk work.
There is no “ethnicity gene”. There are no genes found only in one broad ethnic group, although there may be small, localized genetic variations.
It also reminds us that there is no “disease gene” for most diseases.
Most chronic diseases and physiological processes are polygenic. To date, genetic factors appear to explain only about 2-3% of high blood pressure cases.
Lifestyle factors and body composition (i.e., body size and amount of body fat / lean mass) are much more important, as are broader social, economic, and political determinants of health (such as where people live, what resources they can access, or the discrimination they may face).
Even if there were a clear genetic basis for certain diseases, such a genetic basis might require a particular environment (such as one with pollution or easy access to high-sodium, high-sugar processed fast foods) to be expressed.
What this means for you
- Regardless of your biological sex or genetic ancestry, monitor your blood pressure and other risk factors, especially as you get older. High blood pressure is a risk factor for many other diseases, such as cardiovascular diseases. But it doesn’t act alone. It works with other lifestyle factors.
- Ethnicity is one factor that may change your risk of chronic diseases, whether because of inherited genetic or social factors. Get regular checkups where possible.
- Control the factors that you can control. You can’t control your genetic ancestry. But there are many ways to reduce your risk of high blood pressure, such as:
- eating fewer processed foods, which tend to be high in sodium;
- drinking less alcohol;
- getting regular exercise; and
- maintaining a healthy body weight.
- Recognize that other factors may contribute to high blood pressure. Stress is one of the biggest. If you belong to a group that has traditionally been marginalized in society, recognize that you may feel extra stress thanks to daily-life discrimination and prejudices. (Unfortunately, you probably already know this, though.)
What’s up next: Metabolism
Now that you’re thinking about blood pressure, you might also be wondering about other metabolic factors. Perfect timing!
In the next chapter, we’ll give you an overview of metabolism, and look at some of the processes that can be affected by genetic factors.

