When Susan first came to see me, she wanted an intense diet plan.
She weighed about 260 pounds—and she longed to part with more than 60 of them as fast as possible.
She was ashamed, frustrated, and angry.
“I had my thyroid tested,” she told me. “My doctor said it was low-normal—nothing to worry about. But I think it’s why I’m struggling.”
Her words? I’d heard them before, almost verbatim, from so many women with hypothyroidism (the medical term for an underactive thyroid).
Susan wanted me to tell her how to change her eating habits to lose weight—and she wanted something that would work quickly.
But I knew that until she quieted her negative self-talk, reduced her stress level, made peace with her body, and gained a sense of control, she would struggle with any diet or exercise plan I gave her.
So before suggesting specific nutrition and lifestyle strategies, I set out to help her transform her mind.
Later in this article, I’ll explain exactly how she made this critical mindset shift—and most importantly, how you can help your clients do the same. This new mindset can then form the foundation for those lasting habits that lead to weight loss, energy, and soaring health.
But first, let’s step back and go over some basics.
(Want more deep insights and helpful takeaways on the most important health, nutrition, and coaching topics? Sign up for our FREE weekly newsletter, The Smartest Coach in the Room.)
++++
What is hypothyroidism?
Your thyroid, a tiny gland in the middle of your lower neck, makes hormones that regulate metabolism, energy level, and heart rate, among other things.
When someone has hypothyroidism, the gland doesn’t produce enough triiodothyronine (T3) or thyroxine (T4), so everything slows down. This leads to symptoms like:
- Cold intolerance
- Fatigue
- Dry skin and hair
- Forgetfulness
- Brain fog
- Depression
- Irritability
- Constipation
- Menstrual irregularities
- Fertility problems
- Yellowing of the skin
- Hair loss
- Brittle nails
- Muscle cramps
- Low libido
- Puffiness in the hands and face
- Difficulty losing weight
- Weight gain
Susan? She dealt with at least half of those symptoms on a daily basis.
No wonder she came into my office feeling tired, frustrated, and betrayed by her own body.
Hypothyroidism is most prevalent in women.
Women are five to eight times more likely to be diagnosed with hypothyroid than men, possibly because oral contraceptives, hormone replacement therapy, and the hormonal shifts that take place during and after pregnancy as well as during perimenopause can all boost risk.
Hypothyroidism affects:
- 2 percent of adult women
- 2.5 percent of pregnant women
- 5 to 9 percent of postpartum women
Hypothyroidism is also underdiagnosed.
Up to 60 percent of people with thyroid disease are unaware of their condition, according to the American Thyroid Association.1, 2
That likely stems from a number of issues, including:
- The medical community doesn’t agree on what constitutes a truly “low” functioning thyroid or how and when to prescribe medicine.
- Blood tests for hypothyroid occasionally deliver false negatives.
As for Susan, her blood work put her in a medical gray area. Her thyroid wasn’t making enough T3 and T4 hormones. That was clear.
What wasn’t clear to her doctor: whether her thyroid was slow enough to necessitate medication. He thought the risks of the medicine outweighed the potential benefit.
Susan, of course, felt differently.
Do some people think they have a slow thyroid, but really just… don’t?
Yes. And I usually see this when someone has struggled to lose weight and has hit a stubborn plateau.
I often encourage people to see their doctor and get some blood work done. Because that way, they can find out for sure.
Other than that, however, the process of coaching someone who wrongly thinks they have a slow thyroid is basically the same as coaching someone who really does have one.
In both situations, you want to help the client shift the sphere of control away from the disease and toward what they can personally do: Eat more whole foods, move their bodies, rest and de-stress, and get enough sleep.
There are no toxic side effects to a healthier diet and better self-care. So we’re going to win either way, whether they ultimately have a thyroid condition or not.
Hypothyroidism can lead to a number of serious health problems.
In addition to fatigue and weight gain, a sluggish thyroid can raise risk for:
- Elevated levels of LDL cholesterol
- Heart problems
- Peripheral neuropathy (nerve damage, usually in the legs)
- Infertility
- Frequent miscarriages
- Birth defects
This is why people with hypothyroidism benefit from nutrition and lifestyle changes, even if those changes don’t ultimately lead to significant weight loss.
It’s common for people with hypothyroidism to blame their doctors.
After being dismissed by her doctor, Susan was angry, and she wanted to spend a lot of our 60-minute coaching session complaining about her primary care physician.
This, however, wasn’t a good use of her time.
First, regardless of how she felt about her doctor, I knew Susan would greatly benefit from client-centered collaborative care.
When doctors, registered dietitians, nutrition coaches, personal trainers, and other healthcare providers all work together to support a client, the client wins.
Just as important: When people get caught up in placing blame, they tend to resist change.
Susan wanted her doctor to hear her—really hear her—when she talked about her overwhelming fatigue. And rather than scare her with a lecture about diabetes, she wanted him to give her a real solution, specifically a prescription.
But, right now, she couldn’t control any of that.
Instead, I wanted to focus Susan on what she could control:
- Her self-talk
- How she respected, cared for, and loved her body
- What she ate
- How she slept
- What she did to de-stress
- How much she exercised
- What she did to support her efforts, such as bringing in a nutrition coach and personal trainer to help her achieve her goals
I showed her the “Spheres of Control” diagram below.
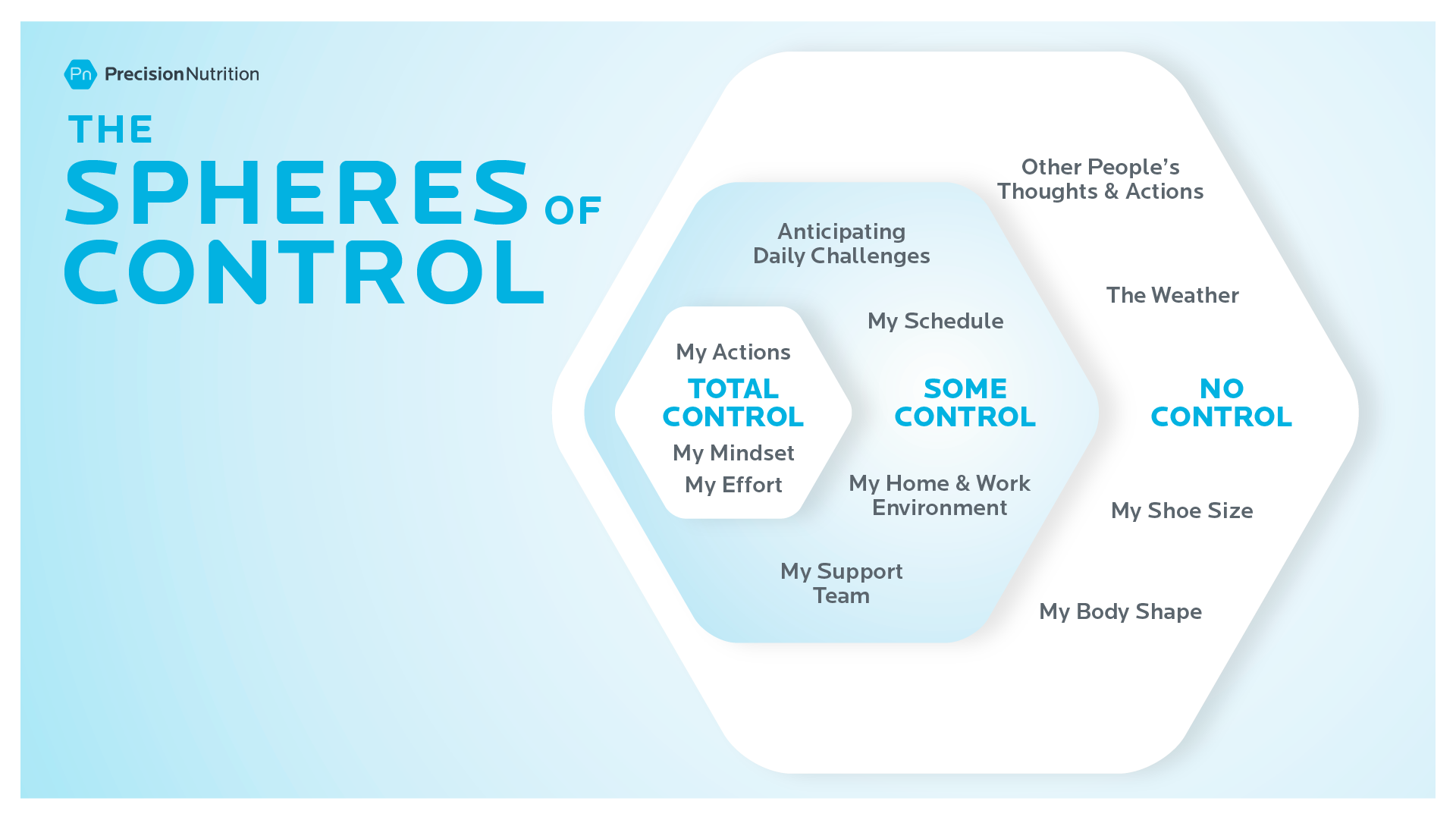
“Let’s consider what’s within your sphere of control,” I told her. “Because you’re much more likely to get support from your medical team if you show that you are helping yourself.”
Something clicked. The anger on Susan’s face began to soften. Her shoulders relaxed, and a curious look came over her face.
“Okay, I guess that makes sense. But what would that look like?”
From there, we worked together to list specific changes that fell into the “total control” and “some control” categories. More on those soon.
Weight loss with hypothyroidism can be a lot harder—and it makes some people want to give up altogether.
Your basal metabolic rate (BMR) includes the calories your body burns to keep you alive: powering your heart beat, growing and repairing cells, adjusting hormones, and breathing.
It accounts for somewhere between 50 to 80 percent of all the calories a person burns. (The rest comes from exercise, digestion, and minor fidgeting movements, called non-exercise activity thermogenesis, or NEAT).
Just how much a sluggish thyroid slows BMR will vary from person to person.
- Someone with no thyroid at all—due to surgical thyroid removal, for example—may experience up to a 40 percent drop in BMR.
- Someone with a functioning thyroid may experience a milder slowdown, in the neighborhood of 6 percent.3-5
For some people, this drop doesn’t make much of a difference, especially if they’re taking thyroid medication. They don’t struggle with their weight anymore than someone without thyroid problems.
But for many others, untreated thyroid issues can reduce the number of calories their bodies burn in a typical day by more than 300 calories. That makes successful weight loss a lot harder.
Someone without thyroid issues might drop a pound or two a week, whereas someone with low thyroid might lose only a fraction of a pound—or not even see the scale move for a week or two.
That’s pretty discouraging, which is why I tend to hear a couple phrases a lot: “Why bother?” and “I don’t even know why I’m trying. It’s hopeless.”
Because of this discouragement, I generally focus on someone’s mindset long before I suggest nutritional or lifestyle changes.
Here’s my step-by-step process.
Save $200 on the industry's top nutrition certification
Help people improve their health and fitness—while making a great full-time or part-time living doing what you love.

Step 1: Address mindset.
Despite what many people believe, a number on the scale just isn’t enough to motivate someone long term. The scale’s readout is also super hard to control.
End result: many people rely on brute force, also known as “willpower.” They think, ‘If I just tried harder, I’d be able to get the scale to move.’
So they tackle a new diet—keto, vegetarian, 100 percent whole food—and they may do okay for a while, but inevitably fail.
Why? Because successful weight loss starts in the mind.
To help get this idea across, I showed Susan “The Iceberg of Success.”

As the iceberg shows, mindset creates a foundation for everything else.
Once someone works on shaping their mindset, it’s much easier to shape their environment: the foods they stock in their kitchen or at work, who they lean on for support, and what they allow themselves to look at online.
For example, continually seeing success photos of a certain friend in a bikini? It’s usually pretty demotivating for someone with a low thyroid.
And once they reshape their environment, it’s a lot easier to change habits: what they eat, how much they exercise, and what time they go to bed.
By tackling change in that order, willpower becomes a lot less important.
In fact, some people can be successful without using much of it at all. That’s why, in the Iceberg of Success, you see willpower at the top—above the level of the ocean.
Once I showed Susan the iceberg, she got it, immediately.
Then, to help her shift her mindset, I used four exercises.
Exercise #1: The destination postcard
Precision Nutrition coaches ask their clients to envision their future. What will their body look like? How will they feel? What will they be able to do?
Then PN clients write a postcard from their future self to their current self. The postcards inspire them throughout their journeys and remind them of their eventual destinations.
I asked Susan, “So let’s start with your destination. Where do you want to go?” I wanted her to envision her life after she reached her goal.
“I want to weigh less than 200 pounds,” she told me.
While Susan was clear about where she wanted to go, I knew the number on the scale was somewhat arbitrary, very much outside of her control, and not likely to motivate her over the long term.
I wanted to shift her mindset to a goal that was intrinsically motivating and also more achievable.
“Okay, but what do you want your life to be like? How do you want to feel?”
She was stumped.
“I don’t see what the point of that is,” she told me. “If I don’t lose weight, my doctor says I’m going to get diabetes. I just need to weigh less than 200. It’s that simple.”
The exercise was a good start, but it was clear that Susan needed more to shift her mindset, so I changed direction.
Exercise #2: Imagine your aura
Yes, this technique is more than a little woo woo.
But bear with me: I wouldn’t tell you about it if I hadn’t seen it work wonders.
I asked Susan to close her eyes.
“I want you to picture a glowing ball that represents someone’s inner spirit. What would that glowing ball look like if someone exercised regularly with joyful movement, ate healthy foods because they tasted good, felt energetic, slept well, and rested when their body needed it? Describe to me what you see in that glowing ball.”
“Sparkly yellow,” she said.
“Okay, now I want you to picture someone who beats herself up with exercise—who doesn’t even take a day off when she’s sick. She starves herself and then binges on a cheat day. She never relaxes or spends time in nature, and she will do whatever it takes to fit into a size 4. What color is that person’s inner spirit?”
“Oh awful. The color of sludgy green sewage,” she said.
“Now, we all come in different sized packages. But regardless of the size or shape of the body that holds this spirit, which of those two spirits do you want to feed?”
“Duh, the yellow one,” she said.
“Which one are you currently feeding?” I asked.
She was silent. I could tell she understood it in an abstract way. But I wanted to make it more tangible. So we moved on to a third mindset exercise.
Exercise #3: Imagine self-care
I wanted Susan to tackle habit change from a place of self-respect, self-care, and self-love.
So I asked, “What would it look like if you respected your body? Talk to me about that. What does respect mean to you?”
“I guess,” she said, “if I respected my body, I wouldn’t try on clothes that are too small every week and then stare at myself in the mirror so I can see my love handles hanging over the top of my jeans. And I’d probably stop weighing my body every day and calling it names based on whatever the scale told me.”
“Great. Okay, now talk to me about what body respect looks like.”
“Well, I’d probably eat better food because it would make me feel better. And I’d probably go to the gym more because it feels good to move my body. But I wouldn’t put pressure on myself. I’d just make it a habit to go regularly. And maybe sometimes I wouldn’t even go. Like, for me, body respect is ‘I don’t want to go to the gym. I want to ride my bike with my son.’”
And then I asked her the same question, but about self-care. She mentioned, among other things, that, if she was caring for her body, she probably wouldn’t raid the vending machine in the afternoon when she was tired.
Then I asked her about self-love.
“If I loved my body, I wouldn’t hate it for the size that it is.”
That was a beautiful and powerful moment.
“Whatever package you come in, you’re going to feel amazing as a human being if you treat your body with love and respect and care and consideration,” I told her.
Exercise #4: If this happens, then I’ll….
Susan was like so many people with messy lives.
She had messy problems.
And those problems kept getting in her way. She’d try to change. She’d do okay for a while. Then her life would… get messy. She’d pause everything. Then weeks later, she’d try again.
For example, Susan wanted to be a person who packed a healthy lunch every day. But she was a single mother with a full-time job and a small child. Her life was busy. Especially on the weekends.
So sometimes she didn’t get to the grocery store.
Which meant that, on Mondays, she often couldn’t pack a lunch because she had nothing to pack. Instead she’d grab fast food. Then she’d forget about packing her lunch—for the rest of the week.
Another messy problem: Frequently, as Susan tried to get to her favorite exercise class, her toddler would melt down—kicking, screaming, hugging her legs, and throwing himself between her and the door.
She’d miss her class—and then she wouldn’t exercise for a while.
More willpower wasn’t going to get her past this.
Instead, we looked at the roadblocks that she kept stumbling over again and again and we brainstormed alternative options for getting around them. We did this by finishing this phrase: If ________________, then ______________.
Here are two examples.
If I don’t pack my lunch then….
… during my lunch break, I’ll run to a grocery store where I can buy chicken with salad.
If I can’t get to my exercise class then….
… I’ll do one of the 25- or 30-minute circuits my trainer created for me to do at home.
By strategizing ahead of time, Susan was able to solve problems as they came up, allowing her to eat healthy foods and exercise more consistently.
Step 2: Build a foundation.
Fundamental skills provide the largest ROI.
Many people with hypothyroidism want to start with fairly intense and specific dietary changes that they’ve read about on the internet.
These often include elimination diets to rule out food intolerances as well as elaborate supplementation protocols to patch deficiencies.
And though such strategies can be helpful eventually, most people can benefit a lot more from a number of simpler and more basic strategies.
These include:
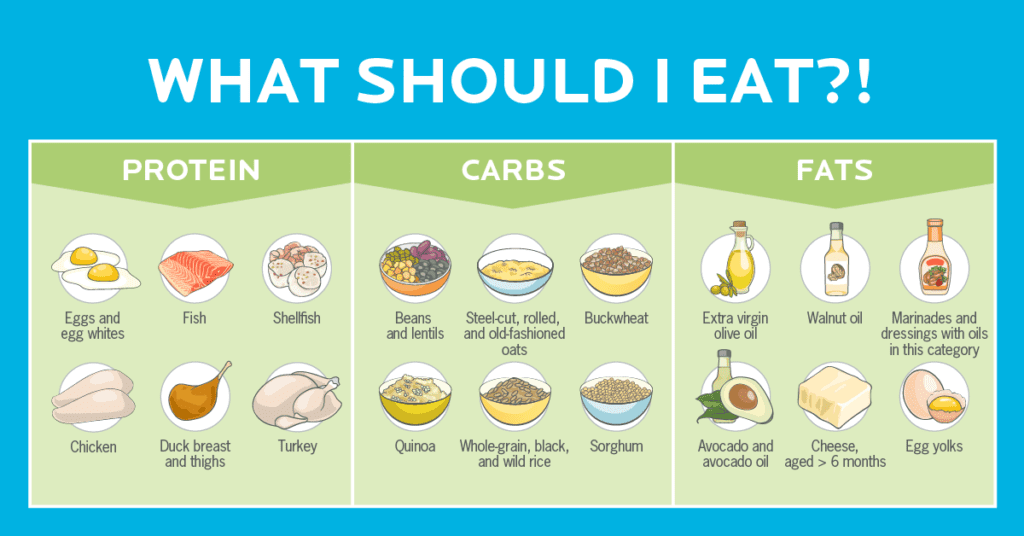
- Eat more minimally-processed whole foods and fewer highly-processed refined foods. This one strategy can help fix most nutritional deficiencies.
- Consume more protein, trying to have a palm’s worth at every meal to reduce hunger and increase satisfaction.
- Prioritize colorful fruits and vegetables, having a serving at every meal, to reduce the inflammation that can signal your immune system to attack your thyroid.
- Shift away from highly-refined carbohydrate foods to slower-digesting smart carbs like beans, legumes, fruit, tubers, and whole grains. This will help to stabilize blood sugar.
- Prioritize healthy fats—such as nuts, seeds, avocados, olives, fatty fish—over other fat sources to help keep inflammation in check.
- Get regular physical activity. Find your sweet spot between pushing yourself—and enjoying it—versus overdoing it and hating it.
- Rest and recover, finding enjoyable ways to reduce stress and relax. Examples: You might enjoy spending time in nature, playing with a pet, getting a massage, or taking a leisurely stroll with a family member.
- Make time for sleep. Create a sleep routine that allows you to drift off quickly, sleep deeply for at least 7 hours, and wake feeling refreshed.
- Build an environment that makes healthy choices easy, for example, by keeping easy-to-grab nutritious foods on hand, such as sliced carrots, apples, and trail mix.
- Tune into your internal sense of hunger and fullness by eating slowly and mindfully, recognizing your sense of hunger and fullness, and stopping when you are 80 percent full, or just satisfied.
If the above sounds like the foundational skills from the Precision Nutrition Level 1 coaching program, it’s because they are.
And, sure, these practices might seem like a big “duh.” Maybe you’re even thinking, “Come on. Tell me something… transformative.”
Here’s the thing: These very simple practices are transformative. Yes, they’re straightforward. But straightforward isn’t the same as easy.
Consider this: How many people do you know who could get a perfect score in 8 out of 10 of the bulleted categories above?
Helping someone master the fundamentals also takes time, creativity, lots of listening, and even more patience.
But the payoff? It’s huge.
These strategies alone can help people lose a significant amount of weight, regain energy, and feel amazing.
They also create the foundation that allows someone to move onto step 3 (coming up next) successfully.
Susan, for example, spent 2½ years building and sharpening these foundational skills until she’d mastered them, consistently using them 80 percent of the time. And they paid off, helping her to lose the first 20 pounds in 14 months. That’s a significant amount of weight—roughly 10 percent of her starting body weight.
She still had a long way to go, however, to reach her goal, which brings us to step 3.
Is there such a thing as a perfect hypothyroidism diet?
Not really. The same types of changes that help everyone get healthier—for example, more whole foods, more protein—tend to also help people with hypothyroidism improve their overall health, too.
That said, there are three specific diets that people with hypothyroidism may want to explore.
The autoimmune diet: A modified Paleo diet, the Autoimmune Protocol Diet (or AIP for short) eliminates inflammatory foods and potential allergens: eggs, grains, legumes, dairy, nuts, seeds, nightshades, sugar and sweeteners, alcohol, and several food additives. Emerging research suggests that following an AIP dietary approach may alleviate symptoms in people with Hashimoto’s thyroiditis, an autoimmune disease that attacks the thyroid.6
The anti-inflammatory diet: Because inflammation can worsen the autoimmune response in people with Hashimoto’s thyroiditis, an eating pattern that showcases anti-inflammatory foods can be helpful.
The elimination diet: By cutting out certain foods and then slowly reintroducing them, you can quickly get a handle on food sensitivities and intolerances.
Step 3: Target any specific nutrition issues that come up.
Occasionally, an underlying issue stands between someone and continued weight loss. I’ve explored three common ones below.
To determine whether clients have any of these problems, ask them to write down everything they eat for seven days, along with other lifestyle factors:
- how and when they move their bodies
- their stress level
- how they sleep
See “What to Look for in a Food and Lifestyle Diary” (coming up below) to learn how to examine a seven-day food log for clues.
Hidden deficiencies
Several deficiencies can contribute to hypothyroidism. These include:
Iodine: The thyroid gland can’t make enough thyroid hormone if it doesn’t get enough iodine. Thanks to iodized salt, very few people have iodine deficiency, but I do occasionally see it in clients who eat very clean. They usually opt for sea salt, which doesn’t contain as much iodine as iodine-fortified table salt, and eat very little if any processed food, which tends to be a rich source of iodine-containing salt.
Iron: In addition to helping the body make red blood cells, iron is essential in the production of thyroid-stimulating hormone (TSH). Up to 43 percent of people with hypothyroidism also have iron-deficiency anemia.7, 8
Selenium: This mineral helps the thyroid use iodine to create the thyroid hormones T3 and T4. Though deficiency is rare, some people are at a higher risk, including people who’ve had gastric bypass surgery or who have Crohn’s disease or kidney problems.
Zinc: Zinc is found primarily in seafood, which explains why deficiency tends to show up in people who are strict vegans or vegetarians.
Copper: Usually we consume all the copper we need from our drinking water, but someone can end up deficient if they supplement with zinc, for example, by taking a lot of zinc-containing cold medicine. Zinc binds to the same cell receptor sites as copper, so too much zinc can crowd out copper, preventing it from getting where it needs to go.
Tyrosine: This amino acid found in dairy products, meats, fish, eggs, nuts, beans, oats, and wheat, is involved in the creation of thyroid hormones.
No matter which deficiency a person has, I try to help them close the gap by eating whole foods, which are less likely than supplements to create a secondary deficiency.
Goitrogens
Certain foods contain substances called goitrogens that stop the thyroid from absorbing the iodine that it needs to work properly.
These foods include cruciferous veggies like broccoli, cauliflower, kale, and bok choy, as well as peanuts, turnips, grapeseed, cassava, and soy.
It’s important to note that people with hypothyroidism don’t need to avoid goitrogenic foods. They’re not a problem for everyone.
And when they are a problem, the fix is pretty simple. All they need to do is cook these foods, as heating and cooking deactivates most of the goitrogens.
Food intolerances
When Susan hit a plateau at 240 pounds, I suspected a food intolerance, especially because she was consuming a lot of gluten-rich foods as well as complaining about bloating and brain fog.
“Would you be willing to try an experiment?” I asked her. “It seems your body is trying to communicate with you. It’s trying to tell you that gluten doesn’t work.”
She agreed.
And within 8 weeks she was down another 10 pounds.
What to look for in a food and lifestyle diary
To find deficiencies, intolerances, and other issues, I ask clients to keep a 7-day food and lifestyle log. Each day they jot down:
- What they ate
- A stress rating, using a 1 to 10 scale
- The number of hours they slept
- How much and when they exercised
As you and your client look over the log together, consider whether they are:
- Eating enough high-quality minimally processed whole foods such as fruits and veggies, lean protein, healthy fats, legumes, nuts, seeds, and whole grains.
- Getting enough sleep.
- Managing stress effectively.
- Finding that exercise sweet spot between pushing themselves just enough—or overdoing it.
And are they doing all of these things consistently, at least 80 percent of the time?
Not everyone gets to their goal—and that’s really okay.
At some point along their journey, most people hit a huge brick wall.
Too often, when this happens, they keep trying to move forward, thinking, “I need more willpower. I just need to try harder.”
Usually, more willpower isn’t what they need, though. Instead, they need to find a path around the wall.
For some people, that alternate route might be hand portions. Or intermittent fasting. Or more exercise. Or more rest and relaxation. Or maybe it’s just finding ways to be consistent with what they are already doing.
For Susan, it was realizing that her original destination wasn’t where she wanted or needed to go.
After hitting 230 pounds, Susan got a bit obsessive for a while. She restricted calories, eating the tiniest of portions. And she punished herself at the gym, never allowing herself a day off.
To a degree, it worked. She got super close to her original goal, with the scale hitting a plateau around 206 pounds.
But she was miserable. Not with the size of her body, but with what it took to maintain that size.
I worked with Susan to find her “best weight,” a term borrowed from Yoni Freedoff, MD, an associate professor of family medicine at the University of Ottawa and author of The Diet Fix.
Your best weight is whatever weight you reach while you’re living the healthiest life that you actually enjoy.
As it turned out, Susan’s best weight was around 220 pounds. Yes, that was 20 pounds more than her initial goal, but it was also considerably less than where she started.
Is she living in a bigger body? Absolutely. But she’s also incredibly healthy, with normal blood pressure, blood cholesterol, and blood sugar.
And she’s wicked strong.
It was when Susan nailed a new PR during CrossFit’s Grace workout that she knew, for sure, she’d reached her destination. That day she did 30 clean and jerks in record time, beating everyone else at the gym.
Afterward, Susan walked over to her son, who was playing nearby. She looked down to see a picture he’d just drawn. It was of Susan, holding a giant weight over her head.
That picture is now on her fridge, to remind her of her deepest why: to be a healthy role model for her son.
References
Click here to view the information sources referenced in this article.
If you’re a coach, or you want to be…
You can help people build sustainable nutrition and lifestyle habits that will significantly improve their physical and mental health—while you make a great living doing what you love. We'll show you how.
If you’d like to learn more, consider the PN Level 1 Nutrition Coaching Certification. (You can enroll now at a big discount.)

Share