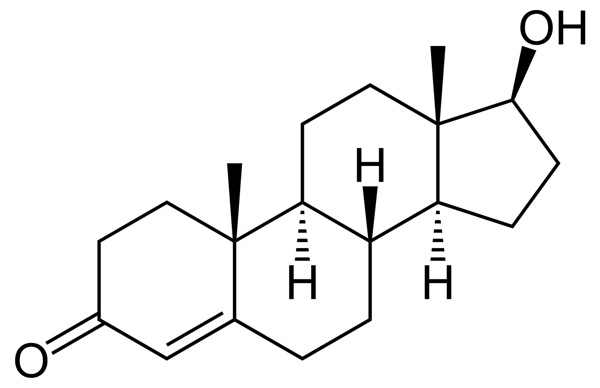
Androgens are a group of steroids that have anabolic (aka growth) and/or masculinizing effects in both males and females. Testosterone is the most important androgen in humans, and regulates libido, energy, immune function, muscle development and bone health.
How is testosterone made?
In males, Leydig cells in the testes synthesize testosterone. In females, the ovaries and adrenal glands synthesize a much smaller amount of testosterone.
Testosterone secretion is controlled by GNRH, which is released by the hypothalamus in pulses. These pulses stimulate the pituitary gland to secrete LH.
LH causes the enzymatic conversion of cholesterol into testosterone in the Leydig cells. Indeed, “cholesterol” has a bad rap in the mass media, but in fact all of our steroid hormones begin with cholesterol. (See chart below.)

Feedback loops
Testosterone, like other hormones, is regulated by a feedback loop.
If the body thinks there’s too much, it “turns off the tap” at the source (i.e. in the brain) or converts the excess to something else such as estradiol or DHT.

Variations in testosterone
Sex differences in testosterone levels
Normal serum total testosterone levels vary from person to person over time, but in general men have much more than women. Typical ranges:
Male: 230-1000 ng/dL
Female: 28-80 ng/dL
Testosterone and age
Testosterone levels increase during puberty from <20 ng/dL to around 300 – 1200 ng/dL at full maturity.
Serum testosterone is secreted in pulses and is circadian. In the second half of puberty, levels are elevated more at night than during the day. During puberty, increases in circulating testosterone and estradiol also induce a much higher secretion (1 ½ to 3 times more) of growth hormone (GH).
Conversely, testosterone levels decline as we age.

Exercise & testosterone
Muscle growth
One of testosterone’s major roles is to control muscle growth.
Androgen exposure throughout early development determines the number and size of motor units. Number, size, and physiological characteristics of motor units determine the size and physiological characteristics of muscle fibres.
Thus, intrauterine androgen exposure may determine our muscles’ ability to hypertrophy (get bigger) in adulthood.
Testosterone release after exercise
Exercise can stimulate a short-term testosterone release, which may amplify muscle growth.
Stimulation of beta-adrenergic receptors encourages testosterone synthesis and release in a dose dependent fashion — the more stimulation, the more synthesis.
Thus, increases in plasma concentrations of testosterone are relative to the intensity of exercise. In other words, the harder you train, at least with resistance exercise or metabolic conditioning, the more testosterone you get.
Scientists think that sympathetic nerve activity and catecholamine secretion — which occur to a much greater extent during, say, a 20-rep squat set than, say, a pleasant stroll — stimulate testosterone during exercise.
However:
- Exercise type matters. Extended bouts of endurance exercise seem to suppress testosterone.
- Sex matters. Plasma testosterone increases occur in men after various forms of exercise, as long as that exercise is high intensity. On the other hand, women respond to intense exercise with very small and/or delayed testosterone increases, or even no testosterone increases at all.
Measuring testosterone
One blood sample is enough to establish circulating testosterone levels, although sometimes doctors may also test salivary testosterone, and if you’re competing in the Olympics, you may find yourself giving a urine test for androgens as well.
Since 98% of testosterone is bound to carrier proteins in the serum (sex hormone binding globulin or SHBG), alterations in these protein levels will change total testosterone levels.
SHBG is produced in the liver and its production is increased by estrogens and hyperthyroidism. SHBG is decreased by androgens, advancing age, and hypothyroidism. Thus, tests may also look for changes in SHBG.
Low testosterone
Several factors can suppress testosterone output and ultimately reproductive function. These factors include:
- chronically low calorie intake (>20% below basal needs) and chronically high calorie intake (especially if obesity results)
- low nutrient intake and vitamin/mineral deficiency
- low fat intake
- depression
- drug use
- overtraining
- limited sexual activity
- stress and anxiety
- aging
- obesity and other metabolic disorders
- overuse of hormonal contraception (in women)
- chronic illness/infection
- poor, minimal, and disrupted sleep (including sleep apnea)
Both men and women can suffer from low testosterone. Symptoms of low testosterone include:
- low energy, fatigue, and lethargy — loss of “mojo”
- decreased strength and work capacity
- low sexual desire, lack of sexual responsiveness and weaker orgasms or difficulty achieving orgasm
- loss of lean body mass, including muscle and bone density, along with an increase in body fat
- increased cardiovascular risk (including poor blood lipid profile), higher blood pressure
Supplementing testosterone
Many athletes supplement testosterone for bigger muscles and/or better athletic performance.
Excessively high doses of testosterone, taken over a long period, can result in:
- acne and oilier skin
- mood changes ranging from hostility to euphoria (though evidence is mixed regarding the prevalence and details, as well as individual susceptibility)
- hair growth (in women) or hair loss
- masculinization of facial features, voice deepening (in women)
- breast growth in males as excess testosterone converts to estrogen
- testicular atrophy in males
- disruption of menstrual cycles in females; increased incidence of reproductive disorders
- certain types of muscle and connective tissue damage
- increased cardiovascular disease risk, including increased blood pressure and heart myopathies along with deep venous thrombosis and embolisms
However, endocrinologists are now starting to prescribe testosterone therapeutically, either for replacement (e.g. in older men and women) or to treat symptoms of many chronic degenerative diseases. The side effects of excessive testosterone listed above generally do not apply to therapeutic and replacement doses.
Summary and recommendations
To maximize testosterone levels for muscle growth, recovery and health:
- Engage in regular, intense exercise sessions
- Don’t severely restrict calories to more than 20% below base needs
- Make sure you are consuming enough micro- and macronutrients
- Engage in safe, regular sexual activity (yes, PN says go get some action!)
- Avoid medications/drugs
- Get adequate sleep, 7-9 hours per night
- Control stress and anxiety levels
Eat, move, and live… better.©
The health and fitness world can sometimes be a confusing place. But it doesn't have to be.
Let us help you make sense of it all with this free special report.
In it you'll learn the best eating, exercise, and lifestyle strategies — unique and personal — for you.
Click here to download the special report, for free.
References
Click here to view the information sources referenced in this article.
Share