What is alcohol?
People have long used chemicals to alter their mood, and probably one of the first substances they used was alcohol.
There are many kinds of alcohol. Ethanol, which is the alcohol found in beer, wine, whiskey, etc. isn’t the same alcohol that the nurse rubbed on your arm before you donated blood — that’s isopropyl alcohol.
Ethanol is formed by the fermentation of plants that are dense sources of carbohydrate (e.g., barley, wheat, corn, fruit). Ethanol is not an essential nutrient and is rich in energy, providing 7 calories per gram.
Alcohol is readily absorbed throughout the entire gastrointestinal (GI) tract, and the rate at which it’s absorbed is likely affected the most by the presence or absence of food in the stomach. After ethanol is absorbed through the GI tract, it heads to the liver, which metabolizes more than 90% of it. The ethanol that isn’t metabolized can enter the bloodstream unaltered.
Indeed, the liver prefers ethanol as a fuel so much that it will displace other substrates when available; in other words, it’ll use alcohol first. Liver alcohol dehydrogenase (LADH) is a rate-limiting enzyme that oxidizes ethanol at ~15 grams per hour (equal to one regular beer). A 70 kg adult male will be legally drunk after four drinks in one hour.
While ethanol itself isn’t toxic, its metabolic byproducts, acetaldehyde and acetate, are. These by-products create nausea after drinking. One drug used to treat alcoholism, called Antabuse, actually allows the concentration of acetaldehyde to accumulate, which results in serious nausea and a strong desire to avoid alcohol in the future. These byproducts can undergo further metabolism or be eliminated via urine or feces.
In the U.S., one “standard” drink provides 15 grams of ethanol, which is found in 12 fl. oz. of regular beer, 5 fl. oz. of wine or 1.5 fl. oz. of 80-proof distilled spirits (e.g., vodka, rum, whiskey). In Europe, a standard drink ranges between 8 and 12 grams of alcohol. “Moderate drinking” is broadly defined as the consumption of about 1 – 2 drinks per day, or up to ~30 grams of alcohol.

Why is alcohol so important?
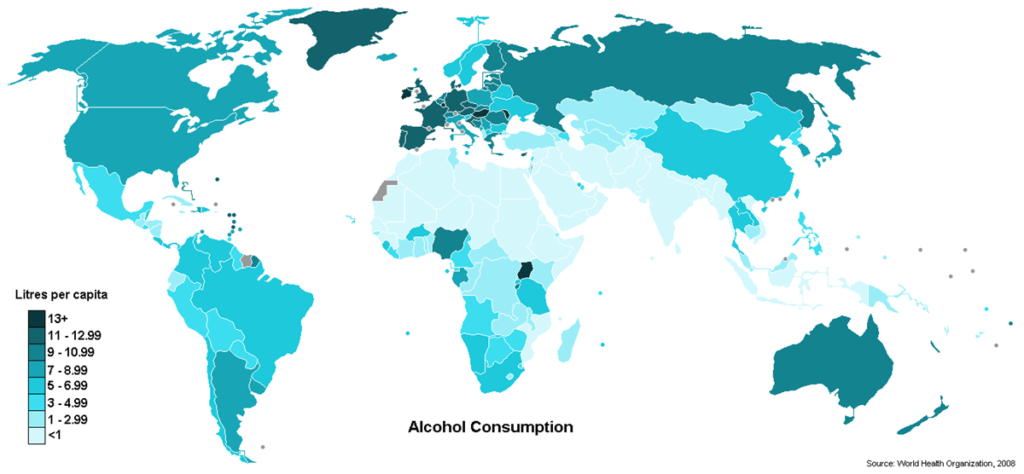
Regardless of the potential health benefits or risks of alcohol consumption, many people use it. Nearly 70% of those above the age of 18 years in most industrialized countries drink alcohol. More men than women use alcohol and intake decreases for both genders after retirement.
A study of 19-30 year olds revealed that 45 percent of men reported heavy drinking in the past two weeks, compared to 27 percent of women.
A small percentage of alcohol users are “problem drinkers.” A dependence on alcohol includes three or more of the following symptoms:
- Drinking despite harm
- Strong desire to drink
- Loss of control over drinking
- Withdrawal symptoms
- Salience (higher priority given to drinking than other activities)
- Tolerance
Alcohol possession and consumption is illegal for those under the age of 21 in the U.S. Nonetheless, alcohol is the most commonly used drug among youth, and 62 percent of American children have tried alcohol by the tenth grade.
Some suggest that alcohol creates social problems. For instance, alcohol abuse costs American businesses an estimated $134 billion each year from alcohol-related illness, on-the-job accidents, and workers’ compensation claims.
Others claim that alcohol is a critical part of a well-functioning society, as the alcohol industry employs millions of people, pays billions of dollars in taxes, and invests billions of dollars in advertising. Research also suggests that moderate drinking may have certain health benefits for some people.
What you should know about alcohol
Alcohol and body composition
There are mixed associations between alcohol intake and body fat. Adding alcohol to one’s usual food intake can lead to obesity if total calories are regularly in excess of daily needs. However, substituting alcohol for one’s usual food intake often leads to muscle loss and protein malnutrition. A large analysis in the U.S. showed that despite a greater calorie intake across increasing levels of alcohol intake, BMI was not increased in women who drank more. Men who drank more than two drinks per day did have a higher BMI than light drinkers. Lack of weight gain in some alcohol users may be due to less food consumption or higher levels of physical activity.
However, as alcohol impairs judgement, people who drink socially may find that they are more likely to engage in problematic eating behaviours while drinking. (A big plate of nachos or chicken wings seems like a great idea by the third beer!)
Alcohol and digestion
Chronic alcohol ingestion impairs pancreatic enzyme secretion, which can result in nutrient malabsorption, particularly of fat and protein. Along with pancreatic digestive function, pancreatic endocrine function can be affected: Insulin resistance is a common side effect of alcoholism, which results in a lack of glycogen formation and energy store depletion. Anaerobic energy production can predominate within the cell, resulting in excessive lactic acid production.
Alcohol and nutrients
Alcohol consumption can alter nutrient status. Alcohol consumption leads to impaired amino acid uptake and protein synthesis in the liver (e.g. lipoproteins, albumin, fibrinogen), along with increased protein oxidation due to necessary cell regeneration. Other compounds, including leptin, are often increased in alcoholics, which can be pro-inflammatory and decrease appetite.
The liver is a major storage depot for vitamins and converts vitamins into metabolically useful forms. Heavy alcohol consumption diminishes the uptake and utilization of folate, vitamin B6, vitamin B1, and vitamin A. Folic acid deficiency is the most common vitamin deficiency among alcoholics, most likely due to the increased demand for nucleic acids needed for regeneration of injured liver cells. Nevertheless, poor dietary intake of folate also contributes. Alcohol acts as an antagonist to vitamin A, vitamin B1, vitamin B3, and vitamin K. Vitamin E has also been depleted in those who consume alcohol.
Alcohol and tolerance
In chronic alcoholics (and regular heavy drinkers; i.e. when alcohol is 10% of total calorie intake or more), a transition is made in the method of alcohol metabolism, from LADH to another oxidizing system. This other system increases alcohol tolerance and lowers caloric output.
Alcohol and hangovers
Alcohol influences blood vessels and fluid volume. This can result in a headache after excessive drinking. Tylenol should never be taken for a hangover headache, as it can interact with ethanol’s byproducts and damage the liver. Nausea is related to the toxic byproducts of alcohol elimination and irritation to the stomach.
Alcohol can suppress anti-diuretic hormone (ADH) release. This means more urine. One standard drink can add 150 mL to urinary output. A few successive drinks can result in a trip to “dehydration-land” (and the restroom).
Alcohol and hormones
Chronic alcohol intake is one of the most powerful mediators of sex hormones. Ethanol is a testicular toxin and can increase the activity of aromatase, an enzyme that converts testosterone to estrogen in the body. Chronic male alcoholics develop an assortment of endocrine disorders, including infertility, gonadal atrophy, and feminization, caused in part by elevated production of estrogens and low testosterone levels. Alcohol abusers tend to have lower testosterone (and LH and FSH).
Alcohol, heart disease and oxidative stress
Moderate alcohol consumption has been associated with health benefits. Data from over 100 studies taking place in 25 countries demonstrates a U- or J-shaped link between alcohol intake and heart disease. This means that the highest mortality is seen among heavy drinkers, with the next highest among abstainers. The lowest mortality is observed among moderate drinkers. One of the reasons that high mortality is seen among abstainers could be due to the “sick former drinker” phenomenon — abstainers are so sick from years of excess alcohol consumption that they must abstain to exist. Also, moderate drinkers may be moderate people, which can lead to improved overall health.
The greatest benefits occur with small amounts of alcohol consumption several times per week, and those with the highest risk of developing heart disease seem to benefit the most. The amount of alcohol that has been linked with the greatest decrease in risk is about one-half to one drink per day. Furthermore, all types of alcoholic beverages seem to offer benefits, not just red wine, which is popular among the public. Still, beverages like red wine may contain other “heart-protecting” compounds.
Excessive amounts of oxidative stress are associated with numerous chronic diseases like cardiovascular, cancer and diabetes. Regularly drinking more than moderate levels (more than ~50 grams per day) can:
- result in higher levels of oxidative stress
- injure the liver
- increase fat synthesis
- displace nutrients (mostly B vitamins)
- displace omega-3 fat intake
- shrink muscle tissue
Obesity is another independent risk factor for liver disease in alcoholics. When muscle is exposed to ethanol on a regular basis, it decreases in size, also receiving less blood circulation and distorted metabolism.

Alcohol and pregnancy
Everyone knows that drinking alcohol during pregnancy is a bad idea, but is it really? The CDC claims that alcohol can cause fetal alcohol disorders, which result in lifelong physical, mental, and behavioral disabilities. Abstaining from consumption makes these ailments 100% preventable. However, some medical evidence has suggested that, as long as no more than one or two units of alcohol are consumed once or twice a week, the baby is unlikely to be affected. The National Health Service of the U.K. states that pregnant women can drink up to 1 to 2 units of alcohol no more than once or twice a week.
Other interesting information about alcohol
- 15% of people who ever use alcohol become addicted (based on a sample of 1200 adults)
- Only 10 – 20% of functioning liver is required to sustain life
- 1 in 4 deaths in the U.S. are due to alcohol, tobacco, or illicit drug use
- We have increased GABA release with alcohol consumption. GABA is an inhibitor. This is one of the reasons that alcohol makes you sleepy at first, but ends up causing a light and easily interrupted sleep.
- Alcohol carries a greater danger of fatal overdose than LSD
- 90 – 100% of heavy drinkers develop fatty liver
- Chronic liver disease and cirrhosis is the 12th leading cause of death in the U.S.
- In the Russian Federation, ~75% of individuals arrested for homicide in 1995 had consumed alcohol
- People that drink alcohol more often increase their level of liver enzymes, this can promote metabolism of certain medications, causing them to be less effective.
- One of the arguments related to alcohol is suicide and depression. The risk of suicide among alcoholics is 50 to 70 percent higher than in the general population. This may be due to the depressive effects alcohol has on the brain, along with its interference on judgment and decision making.
Summary and recommendations
If you aren’t using alcohol, there’s no reason to start. If you are using, then drinking small amounts of alcohol on a regular basis will likely offer the greatest health benefits without promoting fat gain. Any alcohol consumption above low to moderate levels can displace nutrients, increase health risks, and make you act like a degenerate at parties.
Would you take a powerful antibiotic or heart medication without the advice of your physician? Probably not. Still, alcohol is available to virtually anyone who wants it, no prescription necessary. Remember that alcohol is a drug. Be smart.
Further resources
MedlinePlus
Alcoholics Anonymous
CDC & Alcohol
References
Click here to view the information sources referenced in this article.
Eat, move, and live… better.©
The health and fitness world can sometimes be a confusing place. But it doesn't have to be.
Let us help you make sense of it all with this free special report.
In it you'll learn the best eating, exercise, and lifestyle strategies — unique and personal — for you.
.
Share